

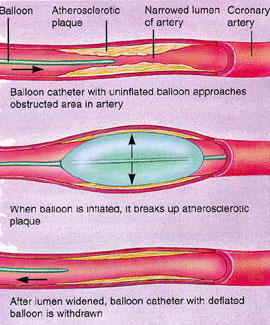
The process is similar to that of a coronary angiogram. However, the catheter (a long flexible tube) has a small inflatable balloon on its tip. This is gently inflated at the site of the blockage so that it squashes the fatty tissue deposits that cause the narrowing against the wall of the artery to reduce the narrowing and improve the blood flow to the heart.
Once a balloon catheter is removed, it may be necessary to place a small wire tube, called a stent, into the artery. The stent expands as the balloon is inflated, so that the stent holds open the narrowed blood vessel. The balloon is then deflated and removed. This prevents narrowings from recurring at the site of the original lesion and maintains the flow of blood to the heart. This procedure may take a little longer than a coronary angiogram.

The preparation and procedure will be very similar to that of a coronary angiogram. You will be given extra blood thinning medication directly into the vein (heparin) and extra tablets to take (clopidogrel) if you are not already taking them. You may also be given a light sedative at the start of the procedure to help relax you during the angioplasty.
The test is performed through an artery at the top of the leg or in the arm. You will receive an injection of local anaesthetic over the artery to numb the area, so it should not be too painful. Once numb, a fine plastic tube (the “guide-catheter”) will be inserted into the artery and passed through to the heart. In order to see the blood flow in the arteries, a special X-ray dye is used that is injected through the catheter into heart. A series of pictures are taken. You will be able to watch the procedure on the TV screens if you wish.
Through the guide-catheter, a fine wire is first passed across the narrowing in the coronary artery. The balloon catheter and stent are passed over the wire to stretch the narrowed portion of the artery. At the end of the procedure the tubes and wires are removed and the puncture in the artery is sealed either by pressure or with a special plug. The procedure usually takes about an hour but may take longer depending on the complexity of the procedure.
Occasionally, people feel mild angina pain during the test, especially when the balloon is inflated to stretch the artery. The pain is transient and usually passes as soon as the balloon is deflated. You should tell the doctor about the discomfort when you get it.
Serious complications are very rare, but because of the nature of the procedure, there is always a small danger. The risks are slightly higher than the risk of an angiogram. The chance of the angioplasty causing a serious complication is less than 1 in 200. Your doctor will not have advised you to have an angioplasty unless he felt that the benefits outweigh this very small risk. You should discuss any worries with him before the test.
The amount of radiation from fluoroscopy used during an angioplasty depends on the length of the procedure, but is considered to be low; and the risk for radiation exposure is therefore low. If you are pregnant or suspect that you may be pregnant, you should notify your doctor due to risk of injury to the foetus. Radiation exposure during pregnancy may lead to birth defects. If you are lactating, or breastfeeding, you should notify your doctor.
For some patients, having to lie still on the procedure table for the length of the procedure may cause some discomfort or pain. There may be other risks depending upon your specific medical condition. Be sure to discuss any concerns with your doctor prior to the procedure.
You should be aware that although the majority of angioplasties are successful, there is a small risk that the procedure may cause a tear in the narrowed artery. Most tears are repaired by the stents that are placed in the artery. If this was not possible for any reason, and if your life was in danger, you may require emergency surgery. A coronary bypass operation would be caried out by a surgeon to prevent serious damage to the heart. Urgent surgery is required in less than 1 in every 200 cases.






